Case of the Month November 2012
This month I would like to address the issue of canal debris and smear layer formation. As an endodontist, I am constantly trying to render a root canal that is not loaded with residual debris, pulp remnants, and, of course bacteria. Several methods have been advocated for smear layer removal. The multitude of solutions and techniques used to produce a cleaner canal preparation are as follows:
1. Preparation design – Step-back, crown-down, double flare, balanced force, modified crown-down, passive step-back, ultrasonic, rotary instrumentation, Self-adjusting file (SAF).
2. Irrigation solutions – sodium hypochlorite in differing concentrations, hydrogen peroxide, saline, local anesthetic, ionized water
3. Chemical means – a chleator either in a cream form applied to the file(RC prep, Prolube, File Eze, Glyde) or an irrigant such as Citric acid, 17% EDTA, Smear Clear, Maleic acid as a final solution prior to obturation.
4. Irrigation solution agitation – Passive ultrasonic, Active ultrasonic (Peizoflow, and there are many others), Tsunami irrigation (Ruddle), Endovac, Continuous Irrigation (SAF).
5: Use of additional irrigants for bacterial removal and canal disinfection – Alcohol, 2% chlorhexidine, Q-mix.
6: Lasers – PIPs
The aformentioned categories are a majority of what has been attempted to produce a canal system in which the residual bacterial load is minimal and there has been a removal of the tissue and debris from lateral canals and canal isthmuses. These, of course, are not all inclusive and there are other steps and solutions that have been attempted.
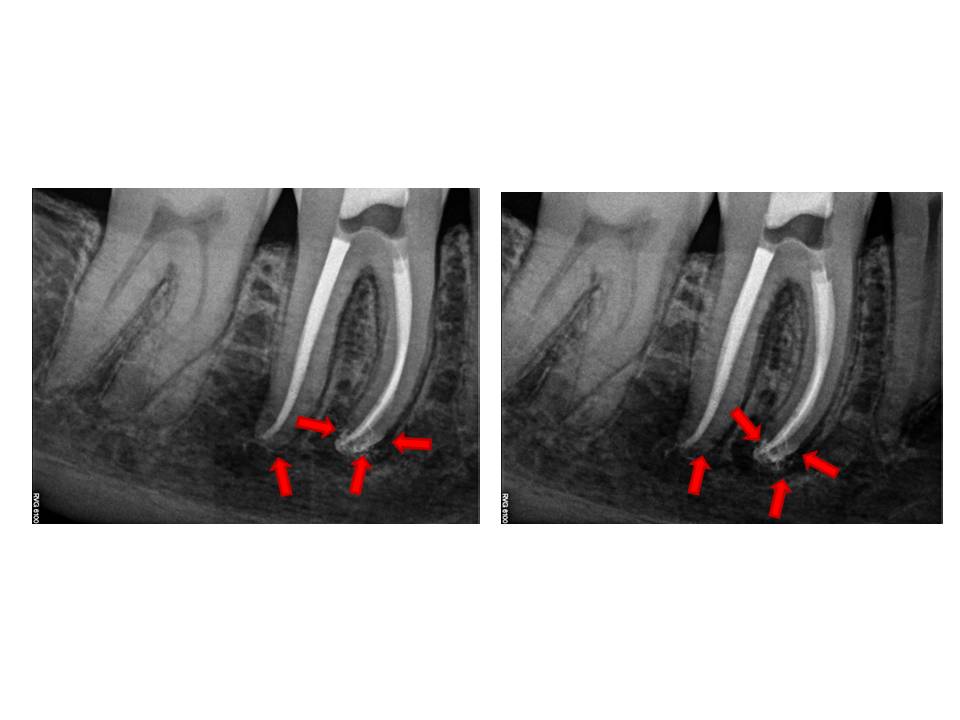
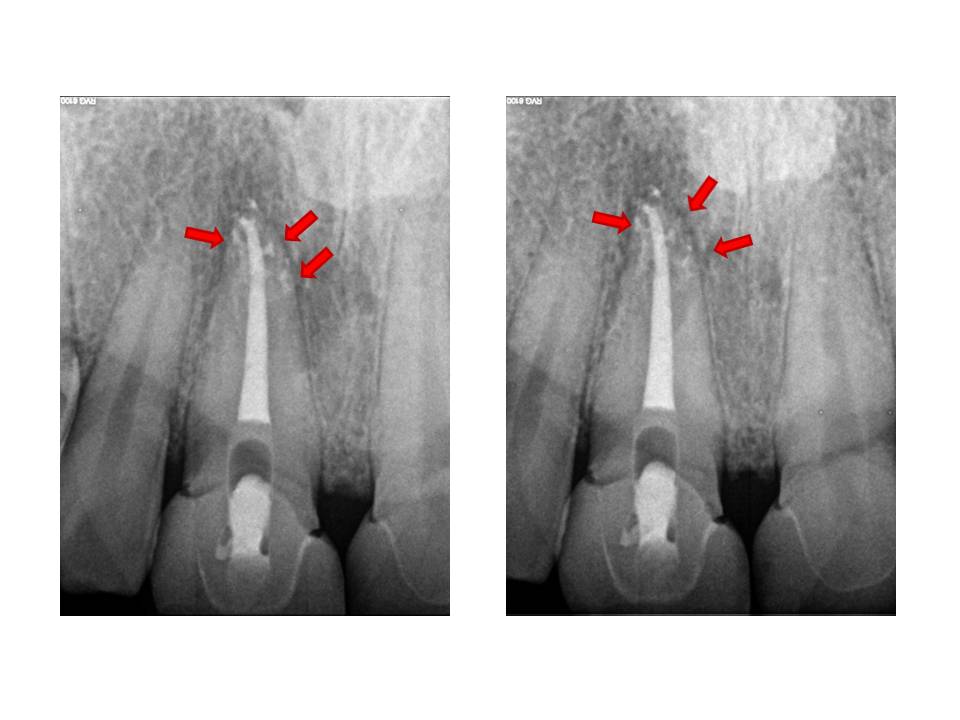
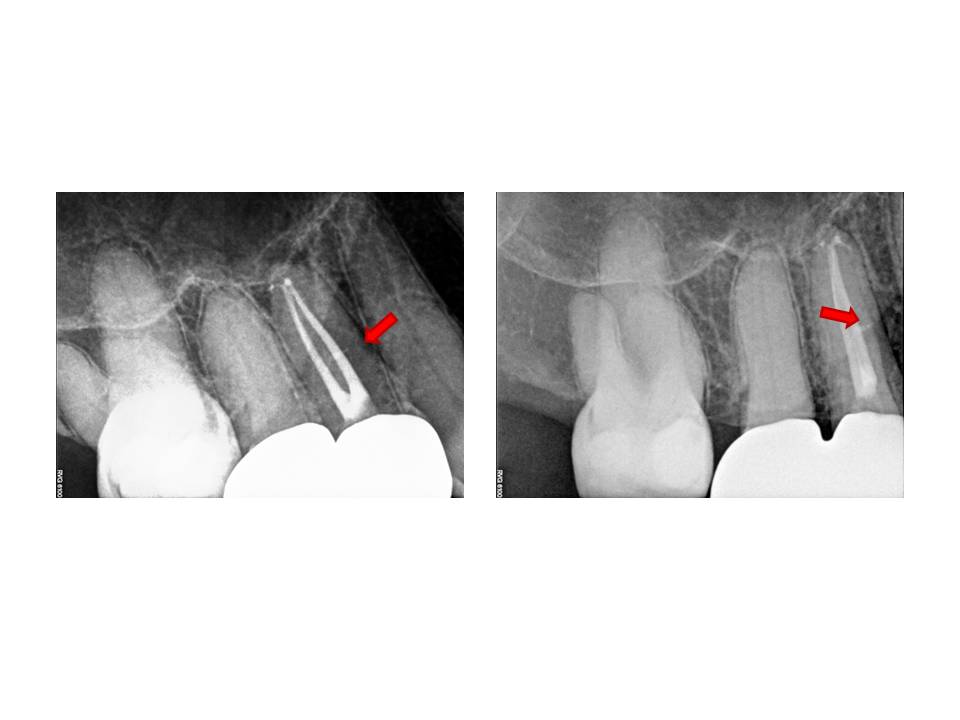
In my experience, and these are my own thoughts, I think that prevention of a smear layer early on during canal preparation is essential. Playing catch-up after debris has been created and packed into the isthmuses and lateral canals is much more difficult to remove. Since I have modified my irrigation routine, I have noticed that the amount of lateral canals that are evident post-operatively, have appeared more often. I offer these examples as support for this change in canal preparation.
In addition to the modification in irrigation, I still use ultrasonic activation of sodium hypochlorite as a final step. By adjusting the thought process of haow the root canal system is approached, I believe we are able to produce cleaner canals and therefore, increased endodontic success. I am open to any questions or thoughts regarding this months post. Thanks again for supporting my practice. I strive to elevate my treatments to the highest possible level.
1. Preparation design – Step-back, crown-down, double flare, balanced force, modified crown-down, passive step-back, ultrasonic, rotary instrumentation, Self-adjusting file (SAF).
2. Irrigation solutions – sodium hypochlorite in differing concentrations, hydrogen peroxide, saline, local anesthetic, ionized water
3. Chemical means – a chleator either in a cream form applied to the file(RC prep, Prolube, File Eze, Glyde) or an irrigant such as Citric acid, 17% EDTA, Smear Clear, Maleic acid as a final solution prior to obturation.
4. Irrigation solution agitation – Passive ultrasonic, Active ultrasonic (Peizoflow, and there are many others), Tsunami irrigation (Ruddle), Endovac, Continuous Irrigation (SAF).
5: Use of additional irrigants for bacterial removal and canal disinfection – Alcohol, 2% chlorhexidine, Q-mix.
6: Lasers – PIPs
The aformentioned categories are a majority of what has been attempted to produce a canal system in which the residual bacterial load is minimal and there has been a removal of the tissue and debris from lateral canals and canal isthmuses. These, of course, are not all inclusive and there are other steps and solutions that have been attempted.
In my experience, and these are my own thoughts, I think that prevention of a smear layer early on during canal preparation is essential. Playing catch-up after debris has been created and packed into the isthmuses and lateral canals is much more difficult to remove. Since I have modified my irrigation routine, I have noticed that the amount of lateral canals that are evident post-operatively, have appeared more often. I offer these examples as support for this change in canal preparation.
In addition to the modification in irrigation, I still use ultrasonic activation of sodium hypochlorite as a final step. By adjusting the thought process of haow the root canal system is approached, I believe we are able to produce cleaner canals and therefore, increased endodontic success. I am open to any questions or thoughts regarding this months post. Thanks again for supporting my practice. I strive to elevate my treatments to the highest possible level.