Case of the month Feb 2011
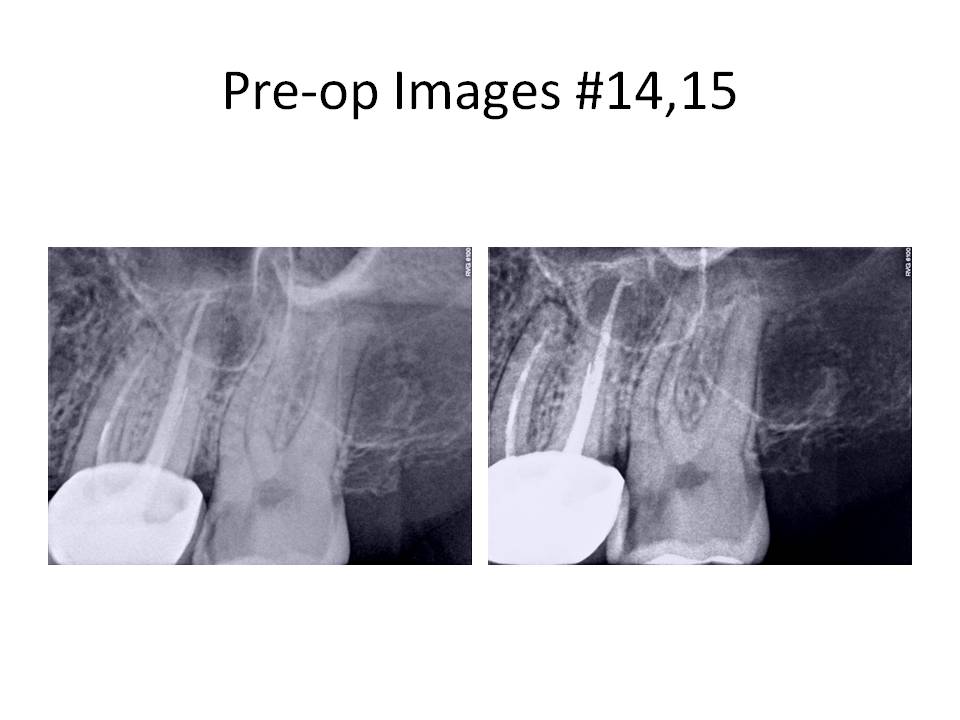
This month’s case is entitled “If you can’t beat ’em, bypass ’em”. The patient is a 29 y.o. female who was referred for evaluation #15 for possible RCT. She was asymptomatic at the time of presentation. Exam revealed gross caries mesially. Pulp tests revealed tooth #15 had a hyperreactive response to cold, normal periodontal probings and negative percussion tenderness. Radiographs revealed normal periradicular tissues and caries that approximated the pulp chamber. Radiographs also revealed that tooth #14 had previous RCT. It was noted that there was a RL lesion associated with the DB root, a separated instrument in the DB root and the canal was instrumented well short of the radiographic apex. Tooth was asymptomatic to percussion and probing depths were WNL. Tooth #14 was treatment planned to have the crn remade by her referring dentist.
The only positive entry in her medical history was Synthroid for hypothyroid. Clinical Dx #15: Caries #15, Asymptomatic irreversible pulpitis with normal periradicular. Dx #14: Previously treated #14 with asymptomatic periradicular periodontitis.

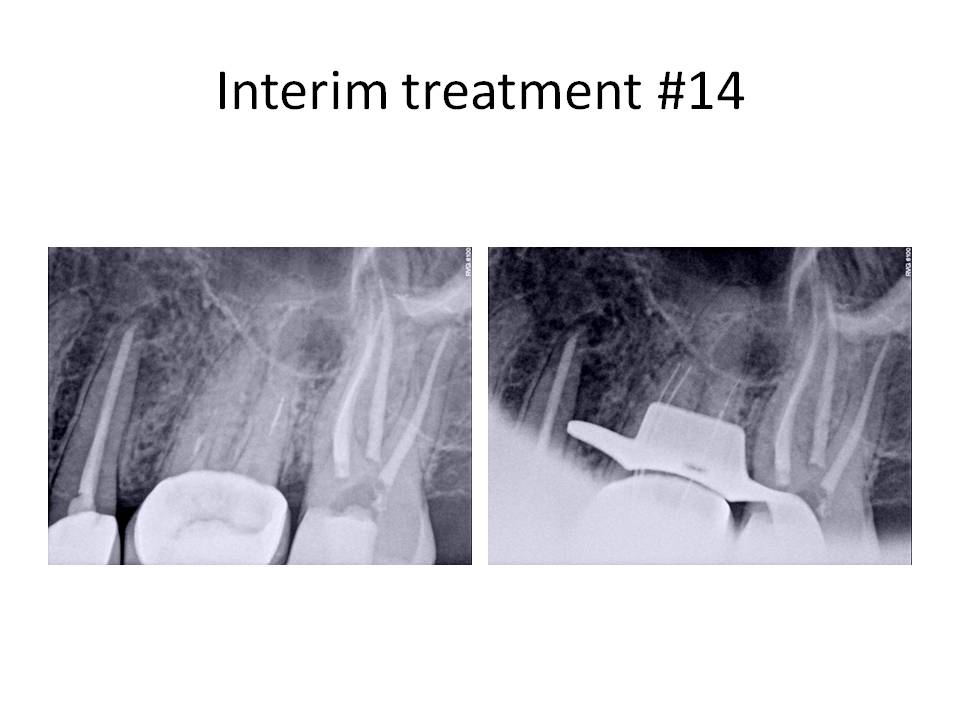
Tooth #15 was treated first. The caries was removed and a vital pulp exposure occurred. The root canal was completed and the patient was appointed for retreatment tooth #14. I will focus on tooth #14 for the remainder of this month’s blog. Tooth was accessed and the Softcore obturation was removed, an untreated MB2 canal was located and instrumented to the apex. An attempt to remove the instrument was not done at this appointment. Calcium hydroxide was placed as an interim medicament and the patient was scheduled to return in 1 week for completion.
At the next appointment, the file was bypassed to the apex and the root canal was completed.
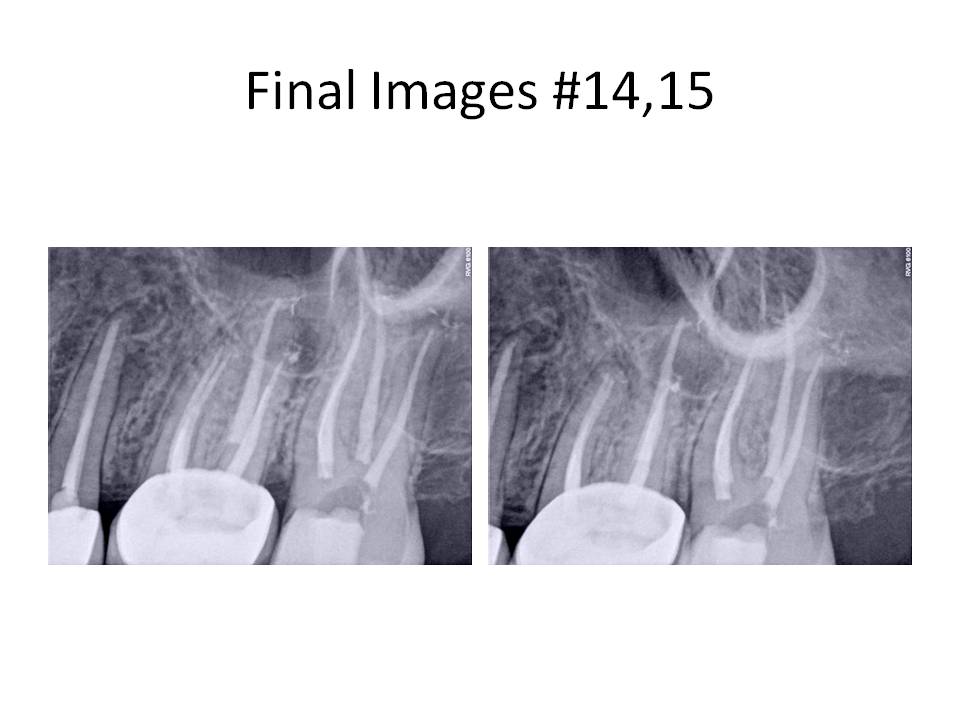
This case demonstrated that sometimes it is easier to bypass a separated instrument, rather than removing it and sacrificing significant tooth structure during the process. There was a higher potential to bypass the instrument than remove it because it was a hand file. Typically, a rotary file is much more difficult to bypass due to its taper. Final radiographs revealed that tooth #13 had a RL lesion present and previous RCT. The tooth will eventually be retreated. I welcome any questions or comments. Thank you for your continued confidence in my practice, Chris
The only positive entry in her medical history was Synthroid for hypothyroid. Clinical Dx #15: Caries #15, Asymptomatic irreversible pulpitis with normal periradicular. Dx #14: Previously treated #14 with asymptomatic periradicular periodontitis.
Tooth #15 was treated first. The caries was removed and a vital pulp exposure occurred. The root canal was completed and the patient was appointed for retreatment tooth #14. I will focus on tooth #14 for the remainder of this month’s blog. Tooth was accessed and the Softcore obturation was removed, an untreated MB2 canal was located and instrumented to the apex. An attempt to remove the instrument was not done at this appointment. Calcium hydroxide was placed as an interim medicament and the patient was scheduled to return in 1 week for completion.
At the next appointment, the file was bypassed to the apex and the root canal was completed.
This case demonstrated that sometimes it is easier to bypass a separated instrument, rather than removing it and sacrificing significant tooth structure during the process. There was a higher potential to bypass the instrument than remove it because it was a hand file. Typically, a rotary file is much more difficult to bypass due to its taper. Final radiographs revealed that tooth #13 had a RL lesion present and previous RCT. The tooth will eventually be retreated. I welcome any questions or comments. Thank you for your continued confidence in my practice, Chris